Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision
making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from our readers and the question was
My Mom is in ICU with Tracheostomy and Whilst Being Weaned Off the Ventilator. How Can I Keep my Mom in ICU Despite Their Plans to Send Her to LTAC?
You can check out last week’s question by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED” I want to answer questions that we get quite frequently as part of my 1:1 consulting and advocacy service!
Why Freezing People After Cardiac Arrest Can Save Lives?
How devastating to think that someone is on the brink of losing one’s life, it could be much worse If you know they are still alive but in a state of coma and can never tell their fate. Or God forbid, having lost someone you love because of sudden cardiac arrest. Clinical studies and innovations nowadays are evolving each time so that most people’s lives can be saved.
Cardiac arrest is one of the most common and devastating cardiac and neurological emergency affecting most of the people worldwide. Most of them are being successfully resuscitated but then did not survive in the hospital or are left with severe brain injuries during the heart attack.
Cardiac arrest is the sudden stopping of the heart. When the heart stops, so does the flow of blood and oxygen to the brain. That lack of oxygen and blood can cause brain damage. The longer the heart goes without beating, the greater the chance for permanent brain injury or death.
If these people are not resuscitated, brain cells begin to be irreversibly damaged, and subsequently the person dies. After resuscitation, treatment within the first few hours is critical for avoiding or limiting brain damage and one of which is the cooling therapy or therapeutic hypothermia.
WHY MIGHT I NEED THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST?
Therapeutic hypothermia can help only some people who have had a cardiac arrest.
Some people regain consciousness right after cardiac arrest. These people often do not need this procedure. It is helpful only for people whose heartbeat returns after a sudden cardiac arrest. If the heartbeat doesn’t restart soon, it won’t help.
Therapeutic hypothermia can be a good choice if the heart restarted but you are still not responsive. It can raise the chance that you will wake up.
RECOMMENDATIONS:
- For patients who are comatose in whom the initial cardiac rhythm is either pulseless ventricular tachycardia (VT) or ventricular fibrillation (VF) after out-of-hospital cardiac arrest (OHCA), therapeutic hypothermia (TH; 32–34°C for 24 hours) is highly likely to be effective in improving functional neurologic outcome and survival compared with non-TH and should be offered (Level A).
- For patients who are comatose in whom the initial cardiac rhythm is either VT/VF or asystole/pulseless electrical activity (PEA) after OHCA, targeted temperature management (36°C for 24 hours, followed by 8 hours of rewarming to 37°C, and temperature maintenance below 37.5°C until 72 hours) is likely as effective as TH and is an acceptable alternative (Level B).
- For patients who are comatose with an initial rhythm of PEA/asystole, TH possibly improves survival and functional neurologic outcome at discharge vs standard care and may be offered (Level C).
- Prehospital cooling as an adjunct to TH is highly likely to be ineffective in further improving neurologic outcome and survival and should not be offered (Level A).
Studies found strong evidence that for patients who are treated with electric shocks to the heart after out-of-hospital cardiac arrest and who are in a coma, cooling body down to 89.6 to 93.2 degrees Fahrenheit (32 to 34 degrees Celcius) for 24 hours, which is called therapeutic hypothermia, is effective in improving their chance of recovering brain function.
It also found moderate evidence that keeping the body cooled down to 96.8 degrees Fahrenheit (36 degrees Celcius) for 24 hours followed by rewarming to 99.5 degrees Fahrenheit (37.5 degrees Celcius) over 8 hours, which is called targeted temperature management, is also effective at helping reduce brain injury after cardiac arrest.
WHAT HAPPENS DURING THERAPEUTIC HYPOTHERMIA?
Therapeutic hypothermia occurs in three phases—induction, maintenance, and rewarming. Clinicians must control hypothermia and rewarming to prevent potential adverse effects, such as arrhythmias and skin breakdown during the cold phases (induction and maintenance)
and rapid electrolyte shifts during the rewarming phase. Temperature should be monitored with a method that measures core temperature, such as use of an esophageal, bladder, or pulmonary artery catheter.
- INDUCTION PHASE
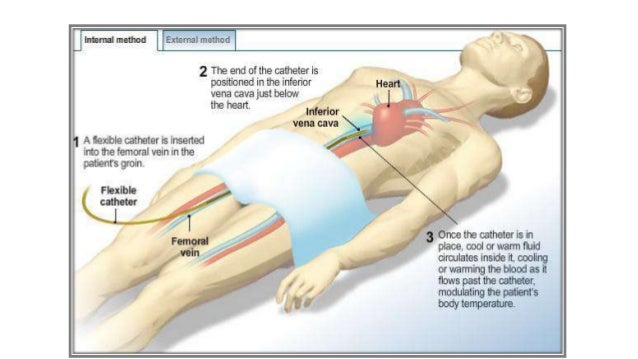
The goal of the induction phase is to get the patient to target body temperature as quickly as possible. Doing this may entail the use of ice packs, iced lavage, rapid cold-fluid infusion, noninvasive cooling devices (such as cooling blankets, wraps, or gel pads), or an intravascular catheter that circulates cold fluid in a closed loop within a large vein. A combination of Rapid cold-fluid infusion with a non-invasive gel pad system
is used.
This phase calls for sedation and neuromuscular blockade when the cooling process begins, to prevent shivering during induction; this allows rapid cooling to target temperature.
- MAINTENANCE PHASE
During the maintenance phase, controlling the patient’s temperature within the target range (usually 32° to 34° C) is crucial. This phase can last up to 24 hours from the time the target temperature is reached (depending on facility protocol). Automated invasive and noninvasive methods can be used to keep the patient within range; these methods are much less labor-intensive than nonautomated methods.
- REWARMING PHASE
Temperature control remains important during rewarming. Warming the patient too quickly or allowing continued shivering causes dangerous electrolyte shifts, leading to potentially lethal arrhythmias. Controlled rewarming of 0.15° to 0.5° C per hour is recommended. To maintain tight temperature control throughout rewarming, the protocol calls for a neuromuscular blockade.
Because electrolytes shift out of the cells back into the serum during rewarming, frequent electrolyte monitoring is needed during this phase to prevent critically elevated levels. Slow, controlled rewarming allows the kidneys to excrete excess potassium, preventing hyperkalemia.
The patient may become hypoglycemic during rewarming as the insulin resistance of earlier hypothermia phases diminishes. Glucose levels must be monitored frequently, with insulin titration and dextrose boluses used as needed to maintain the patient within ordered ranges.
Careful fluid monitoring during rewarming is crucial because of the vasodilation that accompanies a body temperature rise. Volume replacement may be needed to prevent fluid deficit and hypotension.
WHAT ARE THE RISKS OF THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST?
Therapeutic hypothermia is very helpful for some people. But it has some rare risks. Some of these risks include:
- Blood is less able to clot. This can cause bleeding.
- Electrolyte and metabolic problems
- Raised blood sugar levels
WHAT HAPPENS AFTER THERAPEUTIC HYPOTHERMIA AFTER CARDIAC ARREST?
Patients will be in the intensive care unit and they will be carefully monitored by the ICU team. You may be on a ventilator to help with breathing. Patients may need central line and an arterial line, and may be started with inotropes/ vasopressor to support body
functions.
An induced coma is generally required if one requires mechanical ventilation with a breathing
tube to be able to tolerate the breathing tube in their throat and an effective ventilation therapy would be nearly impossible to achieve. Paralyzing agents like Cisatracurium or Vecuronium are used during the course of this treatment and as soon as his or her condition allows, after vital body functions have been regained, the patient will be brought out of the induced coma by reducing the sedation (drugs). This is often a gradual process and may take sometime to wash off
the medications in their system. It might take a few hours and sometimes a few days until your loved one is waking up.
Some people do eventually wake up after therapeutic hypothermia. They may not have any lasting brain injury. Others might have some problems with thinking. They will need therapy. Sometimes, cardiac arrest may harm other organs, like the kidneys. You will need follow-up care.
Medical care will depend on the reason for the cardiac arrest and the degree of damage. Other health problems you have will also determine the care you need. You may need medicine, procedures, and physical therapy. Some people might need surgery for heart disease. Other people might need an automatic defibrillator.
REFERENCES:
- Anoxic-ischemic encephalopathy: association of predictors with the vital and functional prognosis of patients
https://dugi-doc.udg.edu/bitstream/handle/10256/9028/TFG%20M.Angels%20Codinach.pdf?sequence=1
- Induced Hypothermia: How Freezing People After Heart Attacks Could Save Lives
https://www.newsweek.com/2015/01/02/induced-hypothermia-how-freezing-people-after-heart-attacks-could-save-lives-293598.html
- Cooling the body after resuscitation following cardiac arrest
https://www.cochrane.org/CD004128/EMERG_cooling-body-after-resuscitation-following-cardiac-arrest
- Cooling cardiac arrest patients may mean better long-term brain function
https://medicalxpress.com/news/2019-10-cooling-cardiac-patients-long-term-brain.html
- American Academy of Neurology, Practice guideline summary: Reducing brain injury following cardiopulmonary resuscitation. Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology, May 30, 2017.
https://n.neurology.org/content/88/22/2141
- Post Cardiac arrest Hypothermia: New AAN guidelines
https://speciality.medicaldialogues.in/new-guideline-body-cooling-after-cardiac-arrest-recommended-in-some-patients/
- Therapeutic hypothermia after cardiac arrest
https://www.americannursetoday.com/therapeutic-hypothermia-after-cardiac-arrest-what-why-who-and-how/
- Therapeutic Hypothermia After Cardiac Arrest
https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/therapeutic-hypothermia-after-cardiac-arrest
- Image from: Therapeutic Hypothermia
https://image.slidesharecdn.com/therapeutichypothermia-140116143331-phpapp02/95/therapeutic-hypothermia-13-638.jpg?cb=1389882962
Kind Regards

{kind=link}