Hi, it’s Patrik Hutzel from INTENSIVECAREHOTLINE.COM where
we instantly improve the lives for Families of critically ill Patients in Intensive Care, so that you can make informed decisions, have PEACE OF MIND, real power, real control and so that you can influence decision making fast, even if you’re not a doctor or a nurse in Intensive Care!
This is another episode of “YOUR QUESTIONS ANSWERED“ and in last week’s episode I answered another question from one of my clients and the question in the last episode was
Proven Strategies: How to keep your loved one ventilated with tracheostomy in ICU
rather than going to LTAC/subacute care!
You can check out last week’s episode by clicking on the link here.
In this week’s episode of “YOUR QUESTIONS ANSWERED“, I want to continue answering the next questions regarding James’ and Christine’s Dad in ICU who’s had a haemorrhagic stroke.
James’ and Christine’s Dad had a brain decompression where they evacuated a large bleed from his brain after the haemorrhagic stroke. And their Dad also underwent a craniectomy (removal of skull) to decrease the brain pressures after the bleed.
James’ and his sister Christine were getting their Dad in one of the best hospitals in the USA, the Cleveland clinic in Ohio.
In the meantime, their Dad
was getting a tracheostomy because he couldn’t be weaned off the ventilator and the breathing
tube.
He also had ongoing seizures due to the stroke and his anti-seizure medications needed to be optimized so he could “wake up” and progress to Neurology Rehabilitation.
In today’s episode of “YOUR QUESTIONS ANSWERED”, I’m talking to James again while his Dad was trying to be weaned off some seizure medications to get him more awake. James can also see the limitations in terms of the
breathing tube/endotracheal tube his Dad was still having and how he would benefit from a tracheostomy!
James wants to know what’s the best course of action in how to get his Dad more awake, how to manage his anti-seizure
medications without being prone for seizures.
Today’s consulting and advocacy session is another excerpt from various 1:1 phone/email consulting and advocacy session with me and the topic this week as part of this series of 1:1 consulting and
advocacy session with me and the topic this week is
How to manage seizures in Intensive Care after a haemorrhagic
stroke!
You can also check out previous episodes of the 1:1 consulting and advocacy questions with James and Christine here
Part 1
Part 2
Part 3
Hi Patrik,
As you know, Dad had the haemorrhagic stroke a couple of weeks back and he’s still ventilated with a breathing tube he doesn’t
like.
CT scan of the brain suggests a large bleed which they have evacuated and they’ve also done a craniectomy to limit the brain pressures.
He’s still having seizures.
My father is currently on Keppra and Dilantin to prevent seizures.
They did not give him the Keppra last night and he
was more alert. They gave it to him this morning and he does not seem as responsive.
I will find out the dose. Obviously, we need him to wake up so we can get him off ventilator.
Blood pressure medications to heart were removed to regulate his BP and machine to monitor his fever was removed.
BP is 100/50
My father is not very responsive.
My father is on sodium Chloride, Keppra, Antibiotics.
They discontinued the Dilantin (Phenytoine).
He seems like he is sleepy but still moving.
Trying to wake him up because we have to decide on tracheostomy and feeding tube by
tomorrow.
What are your suggestions and thoughts?
James
Hi James,
Please see my responses below in red.
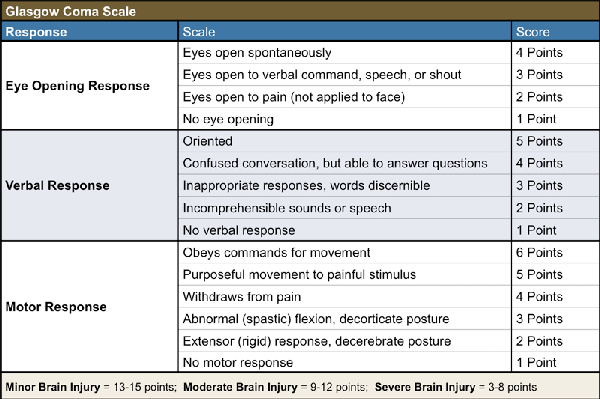
My father is not very responsive. > What does that exactly mean? Is he opening eyes? Is
he still trying to pull out the breathing tube? I understand one side(right side?) is paralyzed and he’s only moving his left side. Can you ask the doctors/nurses about his GCS = Glasgow coma scale? I have attached a picture in relation to GCS. I would imagine your Dad’s GCS might fluctuate between 5-11.
Have a look and ask them. If you need clarification we can discuss over the
phone.
My father is on sodium Chloride. > That is normal standard infusion to keep him hydrated.
Keppra> Keppra needs to be seen in combination with Dilantin (Phenytoine), usually one or the other is given to manage seizures in the beginning. I’m glad they took Dilantin off and only continue with Keppra. One or the other is
fine normally. Keppra has some sedative effect but should not stop Patients from waking up. If your Dad is still not waking up it’s most likely not the Keppra and I will explain in more detail further below
Antibiotic. > Why is he on Antibiotics? Does he have an infection? Did you mention Pneumonia?
They discontinued the Dilantin. > That’s good as long as they can control the seizures
He seems like he is sleepy but still moving. > The movement is a good sign, the sleepiness is part of the head injury and/or seizure medication. Probably a combination of both. The “waking up” in ICU especially after head and brain injury will take time. How much time? I don’t know, maybe days, weeks and maybe even months. That’s why a tracheostomy is the way forward to have a secure airway that’s painless. A tracheostomy will buy your dad time and it’ll be easier to get him out of bed and mobilize him. The more stimulation he can tolerate the better.
I will refer to
some resources below.
Trying to wake him up because we have to decide on trachea and feeding tube by tomorrow. > At this stage from what you are describing, if his neurological condition hasn’t changed since we spoke yesterday and if it’s not significantly changing today or tomorrow, I would suggest a tracheostomy because your dad will be more comfortable with it.
Suggestions ?? > Other suggestions are to get the helmet fitted so they can start mobilizing him once he has the tracheostomy. Please also ask them for his GCS score, I have attached a picture here so you know what it means.
Please have a look at this resource here as well (Normally I sell this EBOOK that comes with 2 videos and 2 audio recordings for
$27)
THE 10 THINGS YOU DIDN’T KNOW ABOUT SEVERE HEAD OR BRAIN INJURIES (INCLUDING TRAUMATIC BRAIN INJURY AND STROKE) IN INTENSIVE CARE THAT YOU MUST KNOW, ESPECIALLY IF YOUR CRITICALLY ILL LOVED ONE ISN’T WAKING UP OR IF
THE INTENSIVE CARE TEAM IS SUGGESTING A POOR PROGNOSIS OR EVEN WORSE, IF THE INTENSIVE CARE TEAM SUGGESTS A “WITHDRAWAL OF TREATMENT” OR A “LIMITATION OF TREATMENT”
Kind Regards
Patrik
Related articles/videos:
Hi Patrik,
My father had a
partial seizure on the left, which is his injured side, this morning.
They started him on Vimpat. Still weaning the Dilantin (Phenytoine).
He is still on Keppra.
Can you please advice?
James
Hi
James,
that’s not so good but also not overly surprising.
Have they done a CT scan of the brain after the seizure?
It also
depends how big and how long the seizure lasted?
Do you know if they’ve given your Dad some Midazolam (Versed) or Diazepam to manage the seizures?
If they are weaning the Dilantin and he’s having seizures, they may need to either wean it slower or increase the Keppra.
It also depends on how much he is stimulated during the day and also the
night.
I’m glad to hear he’s not on any inotropes/vasopressors or vasodilators.
This again is a good sign and it means he’s “only” on one form of major life support the
ventilation.
Great if he can breathe without the tracheostomy, I would be all for it, however the absence of a spontaneous cough will make it very difficult to protect his airway without the tracheostomy.
Recommended:
If they think he will wake up in the next few days and can breathe and cough, it would be tremendous!
Any questions please
let me know.
Kind Regards
Patrik
Hi Patrik,
My fathers blood pressure is 92/46. Seems low.
Temp is 99.9F (37.7C)
Heart rate is
90.
I’m worried.
Can you please advice?
James
Hi James,
Low blood pressure.
He may need inotropes/vasopressors and/or fluid replacement.
Remember 2 steps forward one step back.
Temperature slightly up but not too much.
His heart rate 90 is OK.
If his temperature and heart rate keep going up and his blood pressure going down, he might have an infection.
Recommended:
Other things to look for are infection markers in the blood such as CRP and white cell count. Just ask.
Let me know when you want to get on the phone
again.
Best wishes,
Patrik
Watch out for the next consulting session with James in the next episode of “YOUR QUESTIONS ANSWERED”
See you then!